UPCOMING EVENTS


ASIPP ON-DEMAND VIDEOS

ASIPP MEMBERSHIP
Join ASIPP. Your Voice For Interventional Pain Management

ASIPP has submitted a proposal to the Centers for Medicare & Medicaid Services (CMS) proposing the creation of an Independent Physician Payment Modifier under Medicare.
The proposal is intended to help preserve independent physician practices by establishing a modifier that would identify qualifying independent physicians and provide a 10% payment adjustment for eligible physician services, while maintaining budget neutrality and protecting existing facility payments.
- ASIPP’s Letter to Joseph Albanese, CMS/CM: https://asipp.org/sent-letter-to-joseph-albanese-re-modifier-for-independent-physician-services-7-20-26/
- ASIPP’s Proposed Modifier for Independent Physician Services: https://asipp.org/asipp_proposed_modifier_for_independent_physician_services_07202026/
Conversion Factor: Proposed Cut
With the one-year 2.5% statutory increase for 2026 expiring, CMS proposes:- Qualifying APM participants: $33.17, down from $33.57 (-1.19%)
- All other clinicians (non-QP): $32.84, down from $33.40 (-1.68%)
IPM Codes: Widespread Reductions vs. 2026
Most interventional pain codes are cut 1–6% in the office setting and 1-4% in Facility:| Office Setting | Facility Setting | |
|---|---|---|
| Epidurals (62321 & 62323) | -3.0% to -3.3% | -2.7% to -3.0% |
| Transforaminal (64479 to 64484) | -3.7% to -4.9% | -1.2% to -3.8% |
| Facet joint (64490-64495) | -1.3% to -3.5% | -1.2% to -3.6% |
| Radiofrequency Ablation (64633-36) | -4.9% to -5.2% | -1.2% to -3.3% |
| SCS Lead Placement (63650) | -5.9% | -3.0% |
| EM Services (99203-205, 213-215) | 1.4% to -3.8% | -1.2% to -2.5% |
- Trigeminal nerve injection (64400): -19.9%; greater occipital nerve (64405): -16.6%
- Percutaneous SI joint fusion (27279, facility): -14.9%
- Kyphoplasty (22513–22515): -6.0% to -6.1%
- Spinal cord stimulator trial (63650): -5.9%; percutaneous
- PNS (64555): -6.3%
E/M Services: Major Change to Modifier -25
CMS proposes that when a separately identifiable office E/M visit is billed with modifier -25 on the same day as a 0-, 10-, or 90-day global procedure, only the highest-paid service is paid at 100% — all others, including the E/M visit, are cut 50%. This directly targets the common office-based scenario of a same-day evaluation and injection. CMS also proposes replacing add-on code G2211 with modifier MOD1, valued at 16% of the base E/M code (32% for ACO participants via MOD2). E/M payment rates themselves decline modestly (see attached table).MIPS / Quality Payment Program
- Traditional MIPS would sunset with the CY 2029 performance period (2031 payment year), making MIPS Value Pathways (MVPs) the sole reporting option; three new MVPs are proposed.
- The quality measure inventory would be set at 180 measures (20 removals, 10 additions), with a new MIPS core measure reporting requirement replacing the outcome/high-priority measure requirement (small practices exempt).
- The performance threshold remains 75 points. Separately, the rule proposes refinements to the Ambulatory Specialty Model (ASM), the mandatory model whose low back pain cohort includes interventional pain physicians.
RFI: Duplicate Laboratory Testing, Imaging, and Interoperability
CMS is seeking input on mechanisms to address duplicate laboratory and imaging tests, including MAC edits resulting in non-payment or reduced payment, recoupment of payments, frequency limitations, and revised billing instructions, along with improved result sharing and interoperability. These policies could significantly affect pain practices that rely on imaging and drug testing. ASIPP will submit detailed comments — please send us your input.Act Now
Comments are due September 14, 2026 (file code CMS-1848-P). Please review the attached documents and send your feedback to [email protected] so we can represent you forcefully. ASIPP will fight these cuts, as we always have — but your voice makes the difference.
Updated Facet Joint Intervention
Guidelines Published
The Pain Physician journal has published updated, evidence-based guidelines for facet joint interventions in the management of chronic spinal pain.
Developed by a multidisciplinary panel of 48 authors, these guidelines include 37 recommendations, all achieving 100% acceptance through a modified Delphi process. The recommendations are based on a comprehensive evidence review, with evidence and recommendation strength assessed using modified ASIPP methodology, GRADE, and AHRQ criteria.
The document addresses patient selection, diagnostic facet joint nerve blocks, imaging guidance, radiofrequency ablation, therapeutic facet joint nerve blocks, intraarticular injections, repeat interventions, sedation, antithrombotic therapy, and special safety considerations.
Read the full guidelines: https://www.painphysicianjournal.com/current/pdf/ODE3NQ%3D%3D
CY 2027 Medicare ASC Proposed Rule:
The Good, The Bad, and The Ugly
for Pain Practices
On July 7, 2026, CMS published its proposed rule for the CY 2027 Hospital Outpatient (OPPS) and Ambulatory Surgical Center payment systems (CMS-1850-P). Comments are due approximately 60 days after publication, with a final rule expected in November 2026. Because commercial payers commonly benchmark ASC contracts to Medicare, these proposals will shape both Medicare and private reimbursement. Here is what matters for interventional pain practices operating in the ASC setting.
THE GOOD: Neuromodulation and device-based procedures win big
CMS proposes a 2.4% ASC update, raising the conversion factor from $56.322 to $57.766, and retains the more favorable hospital market basket through 2027. The nervous-system and musculoskeletal specialty groups — home to nearly all IPM codes — each gain +6%, the strongest in the ASC program. Prior authorization for facet injections, facet RF ablation, SCS lead implants, and (starting July 2027) an expanded botulinum toxin list applies only to hospital outpatient departments, not ASCs — making the ASC the faster and better-paid site of service. CMS also proposes adding 618 procedures to the ASC Covered Procedures List.
THE BAD: Bread-and-butter injections keep eroding
Despite the +2.4% system update, epidural injections, facet injections, and facet RF ablation all decline — losing ground to inflation for another year. Office-based payment caps continue to suppress ASC facility fees for many injection codes, and these relative-weight cuts compound annually.
THE UGLY: Cliffs and penalties to plan for
- Non-opioid payment cliff: the temporary separate payment for qualifying non-opioid pain treatments (e.g., liposomal bupivacaine) expires December 31, 2027 unless Congress acts.
- Quality-reporting penalty: ASCs failing ASC Quality Reporting receive only a 0.4% update — a 2-point penalty worth roughly 2% of all Medicare revenue.

In 2026 Telehealth From Your Home Requires You To Enroll Your Home As A Practice Location
We celebrated the extension of Telehealth through next year. During the legislative process and our advocacy efforts, the understanding was that Telehealth flexibilities would continue as they had in previous years. However, a significant change was made that has caught many organizations and practitioners by surprise.
For the past several years, CMS allowed physicians and other practitioners to provide Telehealth services from their homes while billing under their group’s practice address. That flexibility ended on January 1, 2026.
Effective January 1, 2026, physicians and other practitioners must separately enroll each location from which they provide Telehealth services. According to CMS, “virtual-only telehealth practitioners whose only physical practice location is their home address will need to enroll their home address as a practice location.”
This means that:
- If you are currently billing for Telehealth services provided from your home while using your group’s practice address, you should discontinue this practice unless your home location has been appropriately enrolled.
- If you provide Telehealth services in multiple states, you may face significant enrollment and update backlogs, particularly if you intend to enroll multiple practice locations for each physician and other practitioners within your organization.
We encourage all practices to review their Telehealth billing and enrollment processes to ensure compliance with the updated CMS requirements.
https://www.cms.gov/files/document/telehealth-faq-updated-02-26-2026.pdf
ASIPP Sends Letters to Congressional Leaders and CMS Regarding Policies Affecting Independent Practices
The American Society of Interventional Pain Physicians (ASIPP) has sent formal letters to CMS Administrator Dr. Mehmet Oz; Representative, Chairman of the House Energy and Commerce Health Subcommittee; Representative James Comer, Chairman of the House Oversight Committee; and Senator Bill Cassidy, Chairman of the Senate Health, Education, Labor, and Pensions (HELP) Committee.
The letters raise concerns regarding several Medicare policies that may affect independent physician practices and patient access to care, including proposed reductions to practice expense reimbursement, implementation of the Ambulatory Specialty Model (ASM), and physician payment reductions associated with assumptions regarding artificial intelligence-driven efficiencies.
In order to resolve the multitude of issues and protect independent practices into the future, ASIPP is requesting that the following changes are made in the upcoming proposed rule:
- Modification of Practice Expenses of 6 to 11% Cuts for Independent Physicians by Adding a Modifier to Identify Independent Physicians.
- Ambulatory Specialty Model (ASM) – Which is an Unproven Concept Leading to Major Access Issues and Cuts to be Removed as it also Conflicts with ACCESS (Advancing Chronic Care with Effective, Scalable Solutions) Model and WISeR (Wasteful and Inappropriate Service Reduction) Model, and Elimination of Inconsistent ASM Specialty Model Program.
- Reversal of Efficiency Cuts of 2.5% as There is No Efficiency as Studies Show that AI May Help if at All, 20 Seconds Per Note.
In addition, ASIPP sent letters to all relevant committee members in both the House and Senate, including members of the Senate Finance Committee and the Health, Education, Labor, and Pensions (HELP) Committee, as well as members of the House Energy and Commerce Committee and the House Ways and Means Committee.
ASIPP remains committed to advocating for policies that preserve independent medical practices, protect patient access to care, and promote a sustainable physician payment system.
Copies of the letters are available below:
• Letter to CMS Administrator Dr. Mehmet Oz
• Letter to Representative Brett Guthrie
• Letter to Representative James Comer
• Letter to Senator Bill Cassidy
Recognizing 20 Years of Service:
Best Wishes to Melinda Martin in Her Retirement!
 After 20 years with ASIPP, Melinda Martin retired on May 29, 2026.
After 20 years with ASIPP, Melinda Martin retired on May 29, 2026.
Throughout her tenure as ASIPP’s Director of Operations, Melinda contributed to many aspects of ASIPP’s operations and played an important role in supporting the organization’s mission, and educational programs. Her years of commitment and service have been appreciated by board members, faculty, colleagues, and staff alike.
We thank Melinda for her many contributions to ASIPP over the past two decades and wish her all the best in her retirement.
ASIPP Board of Directors Sends Letter to UnitedHealthcare Regarding Medicare Advantage Referral Requirements
On May 28, 2026, the American Society of Interventional Pain Physicians (ASIPP) Board of Directors submitted a formal letter to UnitedHealthcare leadership regarding recently implemented referral requirements affecting Medicare Advantage HMO and HMO-POS plans.
The letter, addressed to UnitedHealthcare Chief Executive Officer Stephen J. Hemsley and Chief Medical Officer Anne Docimo, MD, expresses significant concerns regarding revisions to the referral process that took effect on April 30, 2026.
The letter states that the updated requirements have created substantial administrative burdens for referring physicians and may result in delays, reduced referrals, interruptions in continuity of care, and barriers to medically necessary interventional pain management treatment for Medicare Advantage beneficiaries.
ASIPP requested that UnitedHealthcare reconsider the revised policy and either return to the previous one-time referral process or implement a simplified annual renewal process comparable to prior referral standards.
The letter notes that the current revised process requires referring physicians to enter separate referrals for each individual practitioner within an interventional pain management group practice, rather than allowing a single referral for the practice itself. ASIPP stated that this approach creates unnecessary administrative burdens and may delay timely patient access to care.
The Board of Directors further emphasized that Medicare Advantage plans are required to follow established Medicare coverage policies, including applicable Local Coverage Determinations (LCDs) and national Medicare coverage standards.
Referenced Medicare Local Coverage Determinations include:
- LCD – Facet Joint Interventions for Pain Management (L38773)
- LCD – Epidural Steroid Injections for Pain Management (L39015)
- LCD – Sacroiliac Joint Injections and Procedures (L39383)
The letter also references federal Medicare Advantage coverage requirements under 42 U.S.C. § 1395w-22(a)(1)(A), CMS Medicare Managed Care Manual Chapter 4, Section 10.1, and 42 C.F.R. § 422.101(b).
The Keck School of Medicine of USC has appointed Joshua A. Hirsch, MD, as chair of the Department of Radiology

We are pleased to announce that longtime ASIPP board member Joshua A. Hirsch, MD has been appointed to serve as Keck School of Medicine Department of Radiology Chair with the University of Southern California.
Dr. Hirsch will also be nominated as the holder of the Stewart Dale Fordham, MD, Chair in Radiology at the Keck School of Medicine. Dr. Hirsch was selected from an impressive cohort of candidates in a comprehensive national search. He brings nationally recognized leadership across academic radiology, neurointerventional, health policy, quality, and multidisciplinary clinical operations.
“Dr. Hirsch, who joins us from Harvard Medical School, is a highly collaborative leader who has a track record of strengthening quality and safety, improving operational performance, and aligning clinical services with institutional priorities,” said Carolyn Meltzer, MD, Dean of the Keck School of Medicine.
Dr. Hirsch will continue to serve on the ASIPP Board as an Academic Director on the Executive Committee.
You may learn more about this distinguished promotion by clicking here.
Medicare Advantage Update: Saga Continues
As is widely recognized, Medicare Advantage co-pays continue to increase, while coverage policies are becoming increasingly restrictive. At the same time, CMS continues to provide substantial bonuses to Medicare Advantage plans and appears to be moving toward broader adoption of Medicare Advantage, potentially through automatic enrollment mechanisms that may limit choices for Medicare beneficiaries.
Included below is an update regarding CarolinaEast Medical Center and its decision to discontinue participation with Blue Cross Blue Shield and UnitedHealthcare Medicare Advantage plans. This information was provided by Giovanna Garcia.
CarolinaEast Medical Center’s decision to drop Blue Cross Blue Shield and UnitedHealthcare Medicare Advantage plans after describing payment policies, denials and reimbursement delays as “financially and operationally unsustainable” for the hospital.
CarolinaEast is part of a growing national trend.
Hospitals and health systems across the country are increasingly severing ties with Medicare Advantage plans, citing growing frustration with prior authorization delays, claims denials, and slow reimbursement processes.
- Becker’s Hospital Review reports that 21 health systems dropped Medicare Advantage plans in 2026 amid growing reimbursement and operational disputes.
With Medicare Advantage now covering 55% of eligible Medicare beneficiaries nationwide — more than 35 million seniors — these disputes are becoming increasingly consequential not only for providers and payers, but also for patients who could lose access to care as more hospitals reconsider participation in Medicare Advantage networks.
Providers say the issue is no longer just whether claims are eventually paid — it’s the operational burden required to get paid at all.
- A March 2026 AHA report found hospitals spent $43 billion in 2025 pursuing payments tied up in denials, prior authorizations, and repeated documentation requests.
Many claims are ultimately reimbursed, but only after repeated follow-ups, appeals, resubmissions, coding corrections, and manual intervention across revenue cycle teams.
MedEvolve refers to this growing operational burden as the “denials tax” — the cumulative rework, follow-up activity, and administrative effort required to move claims from submission to payment.
According to Matt Seefeld, CEO of MedEvolve, denial rates alone fail to capture the true operational strain hospitals are facing.
“A denial rate only measures the outcome,” Seefeld says. “It doesn’t measure how much work it actually takes to recover reimbursement. A claim may be reimbursed, but if it required five or six staff interactions to get there, the organization has absorbed a real operational cost.”
Seefeld can speak to what’s driving the growing backlash against Medicare Advantage plans, why hospitals are increasingly describing payer relationships as financially and operationally unsustainable, and how many organizations are beginning to rethink denial rates as a standalone revenue cycle KPI.
Cigna to Cover Spinal Cord Stimulation for Diabetic Peripheral Neuropathy
Diabetic peripheral neuropathy is a covered condition by Medicare and many other insurers however, Cigna has incorporated into the new policy effective August 4, 2026 to cover diabetic peripheral neuropathy when all the criteria are met as follows:
Trial
A short-term trial (i.e., at least [5] days) of a non-high-frequency or high-frequency (HF10 SCS) dorsal column spinal cord stimulator is considered medically necessary when ALL of the following criteria have been met:
- Performed for the treatment of chronic, intractable pain secondary to diabetic peripheral neuropathy in the lower extremities
- Symptoms include BOTH of the following:
- lower extremity neuropathic pain present for >12 months
- pain is rated at least VAS ≥5
- Ineffective pain relief with or intolerance to at least TWO of the following:
- anticonvulsants
- tricyclic antidepressant
- SNRI (serotonin-norepinephrine reuptake inhibitor)
- opioids
- If taking opioids, the opioid use is ≤100MME (morphine milligram equivalent) per day.
- Hemoglobin A1c (HbA1c) <10% within three (3) months prior to trial
- There are no other medical diagnoses (e.g. chronic inflammatory demyelinating polyneuropathy [CIDP]; Hepatitis B; HIV; Lyme disease; chemotherapy or vitamin deficiency induced neuropathy) that are concordant with the presenting symptoms, signs, and results of relevant studies (e.g., imaging, electrodiagnostic testing, laboratory testing, etc.).
- Attestation by a behavioral health provider (i.e., a face-to-face or virtual assessment [with or without psychological questionnaires and/or psychological testing]) reveals no evidence of inadequately controlled mental and/or behavioral health conditions/issues (e.g., substance use disorders, depression, or psychosis) that would impact perception of pain, and/or negatively impact the success of a SCS or contraindicate placement of the device
Permanent Implant
Permanent implantation of a non-high-frequency or high-frequency (HF10 SCS) dorsal column spinal cord stimulator is considered medically necessary when BOTH of the following criteria have been met:
- Must meet ALL criteria for a short-term trial spinal cord stimulator as noted above.
- There has been documented pain relief of at least 50% during a short-term trial of SCS.
ASIPP Sends Letter Supporting H.R. 8163, the Provider Reimbursement Stability Act
The American Society of Interventional Pain Physicians has submitted a formal letter to Greg Murphy, MD, sponsor of H.R. 8163, the Provider Reimbursement Stability Act, expressing strong support for the legislation.
In the letter, ASIPP highlights ongoing concerns related to physician reimbursement and patient access to care, including:
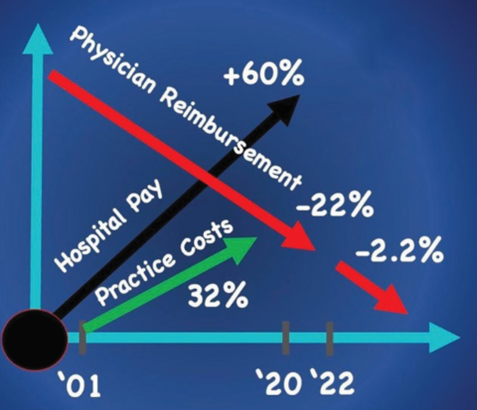
• Declining reimbursement: Physician payment has decreased by 33% since 2001 when adjusted for inflation, with additional 2% sequestration cuts each year and looming 4% PAYGO cuts each year based on the Congressional Budget Office report.
• Rising practice costs: Medical inflation has significantly outpaced general inflation, with healthcare costs increasing by 121.3% compared to 86.1% for consumer goods and services. Practice costs have increased 56% from 2001 to 2025, while reimbursement has declined 33% overall and 41% for interventional pain physicians, with supply costs rising 78%.
• Access to care challenges: Current Medicare reimbursement policies are contributing to the closure of community-based practices, which is reducing patient access to high-quality interventional pain management services—particularly in the ambulatory surgery center (ASC) setting.
ASIPP emphasizes that H.R. 8163 would help stabilize physician reimbursement by modernizing Medicare payment policies, including increasing the budget neutrality threshold, indexing it to the Medicare Economic Index (MEI), and ensuring more frequent updates to practice expense inputs used in RVU calculations.
The letter underscores the importance of supporting independent physician practices to ensure continued access to high-quality, evidence-based pain care.
ASIPP: Why It Matters, What We Do, and How We Lead
Why was ASIPP created—and how has it evolved? This video explores the origin, early development, and history of ASIPP.
Aetna Now Covers Peripheral Nerve Stimulation for Chronic Pain
In a policy published by Aetna last week, entitled Peripheral Electrical Nerve Stimulation for Pain Number: 0011, Aetna describes the coverage conditions for peripherally implanted nerve stimulators as follows:
Aetna considers peripherally implanted nerve stimulators (e.g., Curonix Freedom PNS System, Nalu PNS System, SPRINT PNS System, StimRouter System) medically necessary DME for treatment of members with intractable neuropathic pain when all the following criteria are met.
a. Member has chronic intractable pain, refractory to other methods of treatment (e.g., analgesics and other medications (including TCAs, SSRIs, SNRIs and antiseizure medications, where appropriate), physical therapy (in-person for at least 6 weeks in the past year), local injection, surgery); and
b. Member is not addicted to drugs (per American Society of Addiction Medicine guidelines); and
c. There is no psychological contraindication to peripheral nerve stimulation; and
d. There is objective evidence of pathology (e.g., electromyography/nerve conduction studies and diagnostic blocks of the specific affected nerve(s)); and
e. Trial of percutaneous stimulation was successful (resulting in at least a 50% reduction in pain for a minimum of 3 days). Note: If a peripheral nerve stimulation trial fails, a repeat trial is not medically necessary unless there are extenuating circumstances that lead to trial failure. Trials will be limited to four leads with maximum of 16 contacts.
You can access the updated policy here: Aetna Policy
As you all know, ASIPP has been focused and working on coverage of peripheral nerve stimulators. Enclosed, please see the letter sent to HCSC Policy Review on October 7, 2025.
Humana to Cover Spinal Cord Stimulators for Non-Surgical Back Pain
After numerous attempts by various stakeholders, Humana has issued a policy covering spinal cord stimulators for non-surgical back pain. We are hoping that others will follow suit.
Please see the Humana Coverage Policy, along with ASIPPs letter to Humana related to spinal cord stimulators.
ASIPP Advocacy Update:
Recent Letters on Coverage and Physician Payment Policy
ASIPP recently submitted several letters on key issues affecting patient access to care and the sustainability of independent physician practices.
Clinical Input to Cigna on Peripheral Nerve Stimulation (PNS) Coverage
ASIPP submitted input to Cigna regarding their position on Peripheral Nerve Stimulation (PNS). The letter highlights current clinical evidence, peer-reviewed research, and ASIPP’s evidence-based guidelines supporting PNS as an established treatment option for appropriately selected patients with chronic pain.
ASIPP requested that Cigna reconsider the “not medically necessary” designation for Peripheral Nerve Stimulation, update Policy #0539 to reflect PNS as medically necessary for appropriate indications, and consider precedents from other payers such as Aetna, BCBS Alabama, and Medicare MACs.
Read the full letter:
https://asipp.org/letter-to-cigna-medical-policy-department-re-clinical-input-regarding-cignas-peripheral-nerve-stimulation-pns-medical-coverage-policy-0539-2-11-2026/
Coverage Consideration for the MILD Procedure for Lumbar Spinal Stenosis
ASIPP submitted letters to Elevance Health, Aetna, UnitedHealthcare, Humana, and Cigna supporting coverage for the MILD Procedure (Minimally Invasive Lumbar Decompression) for patients with lumbar spinal stenosis and neurogenic claudication. The letter highlights clinical evidence, FDA clearance, and real-world outcomes demonstrating the safety and effectiveness of this minimally invasive treatment option.
ASIPP also encouraged these payers to adopt favorable coverage policies aligned with newly approved Category I CPT codes effective January 1, 2026, to help ensure patient access to this evidence-based procedure.
Read the full letter:
https://asipp.org/letter-regarding-coverage-consideration-for-the-mild-procedure-for-lumbar-spinal-stenosis-with-neurogenic-claudication-2-25-2026/
Medicare Physician Fee Schedule and Impact on Independent Practices
ASIPP submitted a follow-up letter to The Honorable Chairman James Comer, Chairman, House Oversight Committee; The Honorable Chairman Brett Guthrie, Chairman, Energy and Commerce Health Subcommittee; Senator Bill Cassidy, MD, Chairman, Committee on Health, Education, Labor, and Pensions; The Honorable Chairman Mike Crapo, Chairman, Senate Finance Committee; and Senator Marsha Blackburn regarding concerns about the Medicare Physician Fee Schedule and its impact on independent physician practices.
The letter outlines several policy issues, including proposed reductions to practice expense reimbursement, the need to reinstate broader telehealth access, concerns regarding the Ambulatory Specialty Model (ASM), and the reversal of proposed efficiency cuts tied to assumptions about AI-driven documentation improvements.
ASIPP urged policymakers to examine these issues through hearings and policy review, noting the potential impact on physician reimbursement, patient access to care, and the stability of independent medical practices.
Read the full letter:
https://asipp.org/letter-regarding-follow-up-to-medicare-physician-fee-schedule-damages-independent-practices-letter-1-12-2026/

Telehealth services extended through December 2027
The House and Senate have both passed and the President signed the federal spending package, which includes HHS funding and an extension of telehealth services through December 2027.
This legislation is effective retroactively as of February 1, 2026. As a result, there is no lapse in telehealth coverage that would have otherwise occurred following the January 31, 2026, expiration under the continuing resolution. In addition, the continuing resolution has been extended for an additional two weeks and continues to include telehealth services. We have been advised that there will be no disruption in telehealth reimbursement, and that all claims will be paid retroactively.
Please see the enclosed document for the specific legislative language included in the bill.
Extension of the telehealth provisions has been one of the major focuses of ASIPP’s efforts. Over the past several months, we have worked closely with Chairman Guthrie, Chairman Comer, and Chairman Cassidy to advance this initiative. ASIPP is very pleased to have secured this outcome—while mid-term rather than permanent, the two-year extension provides important continuity and stability. The language remains unchanged, with the extension being the primary modification, as outlined in the enclosed text.
Thank you for your continued assistance and cooperation. We also extend our sincere appreciation to our congressional supporters who helped make this significant achievement possible.
Bibliometric Analysis of Musculoskeletal RFA Research Identifies Dr. Laxmaiah Manchikanti and Dr. Steven P. Cohen as Leading Authors, with Pain Physician and Pain Medicine Among the Most Influential Journals
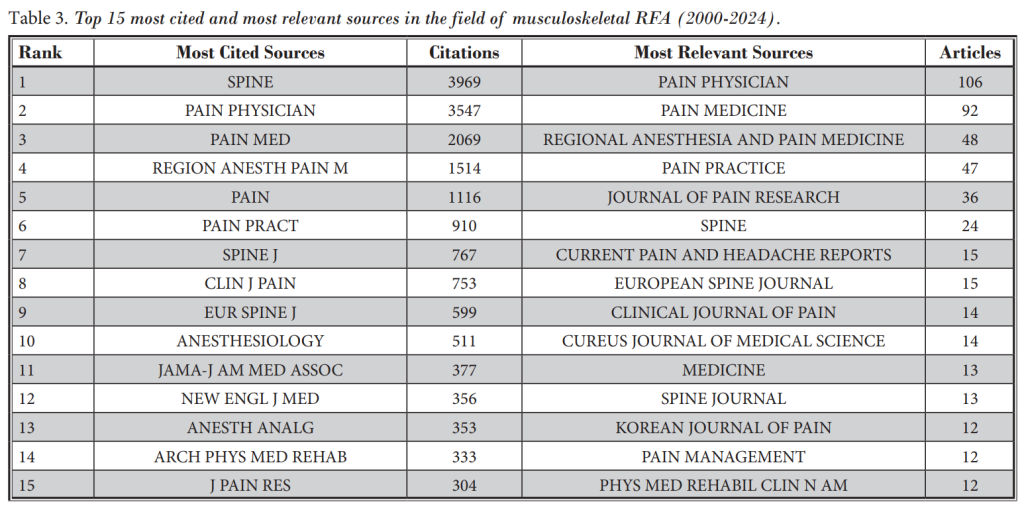
A recent article in Pain Physician titled “Radiofrequency Ablation for Musculoskeletal Pain: A Bibliometric Analysis of Global Research Trends (2000–2024)” (Pain Physician 2025; 28:S157-S168) examines the research landscape surrounding radiofrequency ablation (RFA) for musculoskeletal pain. The analysis identifies Pain Physician as the most relevant journal in this field, with Pain Medicine ranked as the second most relevant source.
Key findings and related bibliometric rankings include:
- Laxmaiah Manchikanti
- Identified as one of the most influential authors based on sustained productivity and citation impact, with contributions shaping the evidence base for spinal and genicular nerve interventions (Pain Physician 2025; 28:S157-S168)
- Ranked #1 globally for randomized controlled trials in chronic pain therapy spanning 1989–2024 (Medicine, 2025; 104:39)
- Ranked #1 among the most cited studies on epidural steroid injections (PM&R Sciences, 2025; 292-297)
- Dr. Steven P. Cohen
- Recognized for high citation impact and influence in musculoskeletal RFA research (Pain Physician 2025; 28:S157-S168)
For detailed data, please refer to the full article:
https://www.painphysicianjournal.com/current/pdf?article=ODA5Mg%3D%3D
ANNOUNCEMENTS
[ INFORMATION | APPLICATION ]

[ MENTOR FORM | MENTEE FORM ]

[ CLICK TO VIEW ]

Doctor Finder allows you to search for an ASIPP® Member Interventional Pain Physician anywhere in America by name or by location. It’s quick and easy.

Leading experts in their respective fields contributed chapters on specific topics to present a cogent and integrative understanding of the field of regenerative medicine as applicable for interventional pain physicians.
[ READ MORE ]
This comprehensive review covers the full and latest array of interventional techniques for managing chronic pain and features new chapters covering challenges with opioid therapy, impact of COVID-19, and spinal interventional techniques.
[ READ MORE ]