UPCOMING MEETINGS & COURSES


[ REGISTER | HOTEL | PROSPECTUS | AGENDA ]
ASIPP ON-DEMAND VIDEOS


ASIPP PODCASTS
Here are some of the available ASIPP® Podcasts:
- A Discussion on Tolerance, Dependency, and PTSD with Dr. Joseph Cabaret and Dr. Kenneth Carle
- Dr. Amol Soin And The Business Side Of COVID-19
- Dr. Kevin Pho of KevinMD.com Reveals Terrific Insight And Ideas On The “New Norm” After The COVID-19
- Andrea Trescot, MD Takes On The Subject Of Controlled Substance Management
- ASIPP® Pod August 2019 – Distinguished Pain Leaders Prunskis, Prunskis, and Helm Discuss Issues That Face IPM
- Miles Day Of Texas Tech Discusses Multiple Pain Management Topics
ASIPP MEMBERSHIP
Join ASIPP. Your Voice For Interventional Pain Management
ASIPP Responds to Damaging BMJ Publications Threatening Patient Access to Interventional Spine Care
The American Society of Interventional Pain Physicians (ASIPP) expresses grave concern regarding two recent publications in the British Medical Journal (BMJ) that risk significantly limiting patient care and choice in the management of chronic non-cancer spine pain.
- Letter from ASIPP President, Christopher Gharibo, MD
- Letter from ASIPP Chairman of the Board and CEO Laxmaiah Manchikanti, MD; ASIPP President-Elect Mahendra Sanapati, MD; and Academic Director, Joshua Hirsch, MD
- Formal withdrawal request
To continue this vital conversation, ASIPP will host a dedicated one-hour session at its 2025 Annual Meeting in Orlando. The session will take place on Saturday, May 17, and will be co-chaired by Dr. Christopher Gharibo and Dr. Nick Knezevic. It will include a 30-minute panel discussion with panelists: Alaa Abd-Elsayed, MD; Salahadin Abdi, MD, PhD; Sheri Albers, DO; Alexander Bautista, MD; Miles Day, MD; Shravani Durbhakula, MD; Alan Kaye, MD, PhD; Sean Li, MD; Laxmaiah Manchikanti, MD; Deborah Tracy, MD; Vinita Singh, MD; and Michael Schatman, PhD. ASIPP invites all to attend this important session. Register here.
ASIPP Advocacy Update: ASIPP Recently Met with Congress to Advocate for Several Critical Issues, Including the Extension of Telehealth Services
We want to update you on our recent visit to Washington where several ASIPP members met with key members of Congress, in both the House and Senate.
We advocated for several critical issues, including the extension of telehealth services. While we were unable to secure a permanent extension, we successfully obtained a six-month extension and will continue working for a long-term solution. Additionally, we are making progress on fraud and abuse legislation which will soon be ready for introduction.
We are also working to eliminate the recurring two-percent sequester cut and address abuses in Medicare in Medicare Advantage Plans.
Finally we discussed coverage for Peripheral Nerve Stimulation and emerging CPT coding challenges. We will be sending you a letter soon regarding ASIPP’s advocacy efforts. We encourage you to join us in these important initiatives.
BREAKING NEWS: Bill Passes House for Telehealth Provisions – Senate Must Approve for a 6-Month Extension
Through ASIPP’s extensive advocacy efforts, we were successful in getting language included in the continuing resolution to fund the government through September. This resolution would extend telehealth provisions for another 6 months.
The bill passed in the House on Wednesday while the ASIPP group was still on Capitol Hill. It appears that the extension is working its way through the Senate for approval. We are encouraged, but it has not yet been finalized.
While this is a temporary measure, our focus remains on securing a long-term solution. Many members of Congress and the Senate are advocating for a more permanent extension, ideally lasting 5 to 6 years or longer. ASIPP will continue pushing for this critical advancement.
We will provide further updates on our Capitol Hill visits and ongoing advocacy efforts soon.
BREAKING NEWS! Pain Medicine Case Reports journal has been accepted for inclusion in MEDLINE and PubMed
The American Society of Interventional Pain Physicians is excited to announce that Pain Medicine Case Reports journal (eISSN 2768-5152) has been accepted for inclusion in MEDLINE and PubMed, the prestigious bibliographic database of the U.S. National Library of Medicine. Pain Medicine Case Reports, a companion publication to the prestigious Pain Physician journal by ASIPP, joins its counterpart in achieving indexing in both MEDLINE and PubMed, marking ASIPP’s dual presence in these renowned databases.
The inclusion of Pain Medicine Case Reports journal in MEDLINE signifies a higher level of selectivity, as MEDLINE consists of the top 5,200 biomedical journals. This indexing also means that articles from Pain Medicine Case Reports will be searchable using NLM Medical Subject Headings (MeSH terms) and other metadata.
The selection for MEDLINE follows a rigorous evaluation process by reviewers from the Literature Selection Technical Review Committee (LSTRC). According to their criteria, the scientific quality of a journal’s content is the primary factor considered for indexing.
We extend our congratulations to the Pain Medicine Case Reports Editor-in-Chief, Deputy Editor-in-Chief, Journal Team, and Editorial Board for this achievement, which underscores the significance and excellence of this esteemed journal.
EXTREMELY IMPORTANT NEWS! Telehealth Changes in the Final Rule 2025 of Physician Payments CMS-1807-F and CMS-4201-F5
Thank you for your attention and participation in various activities in protecting medical practices.
We want to bring to your attention critical issues affecting patients across the United States, including those covered by Medicare, Medicare Advantage, Medicaid, and commercial insurers.
The Medicare Final Rule has significantly changed the provision of telehealth services. Starting April 1, 2025, most telehealth services will require patients to be physically present in an office or medical facility located in a rural area. This restriction excludes patients in non-rural areas from accessing telehealth services altogether. Even for those in rural regions, traveling to a designated facility can be extremely difficult, undermining one of telehealth’s primary benefits—providing care from the patient’s home. These changes will impose substantial transportation costs, create burdens for elderly patients who cannot drive, and disrupt the working population that relies on telehealth for accessible care. Currently, approximately 20% of patients depend on telehealth services.
Furthermore, if this rule remains in place, Medicare Advantage, Medicaid, and commercial insurers are expected to adopt similar policies, likely with reduced reimbursements. This will effectively dismantle telehealth services, severely limiting patient access to essential health services.
This issue is crucial for millions of patients across the country, and we hope you will take action to help preserve access to these vital services. We urgently request you to contact CMS and members of Congress (House and Senate).
Please go to VoterVoice and from there, send your letters. You may also copy the letter into your own letterhead or e-mail it directly. We have created a sample letter for your convenience.
IMPORTANT NEWS! Medicare MACs Will Hold Claims Until January 14 Instead of January 28 as Previously Notified
Some of you may have received notices from Medicare that they will be holding claims until January 28, so that CMS can make necessary claim system updates. Holding them for 28 days is very difficult for providers to cope with.
ASIPP has contacted CMS through our advocacy team of Jeff Mortier and Randi Hutchinson. Chairman James Comer and Senator John Boozman contacted them on our behalf and expressed concern on the policy. Following this, they received a response from CMS stating that they will be holding claims until January 14 instead of the 28th to make the necessary claims system updates, which is part of the normal process.
The following is the full text from CMS:
The MACs are holding claims until January 14th to make the necessary claims system updates, which is part of the normal process when we implement extenders legislation. The MACs should not be denying these claims. CMS has directed the MACs to make any necessary changes before claims are released to pay telehealth claims dates of service 1/1/25 through 3/31/25 with all of the same flexibilities that applied to telehealth and related services for 2024. In addition, if any claims were processed incorrectly, the MACs have been directed to automatically adjust the claims.
CMS is also actively working to update public-facing information to ensure health care providers and beneficiaries are aware of the temporary extension.
We hope this information will be helpful to you. If you have any issues for beyond January 14, please feel free to contact us so we can contact CMS.
Updated Information on the 2025 Medicare Physician Fee Schedule
Peripheral Nerve Stimulation
Guidelines Available!
The Evidence-Based Clinical Guidelines for the Use of Implantable Peripheral Nerve Stimulation in the Treatment of Chronic Pain from ASIPP are now available! This 92-page publication includes 374 references, 20 tables (plus 8 appendix tables), and 9 figures.
These guidelines support the use of implantable peripheral nerve stimulation leads and neurostimulators in patients with moderate to severe chronic pain refractory to two or more conservative treatments, and aim to optimize patient outcomes and promote health equity through the integration of PNS technology in clinical practice.
Find the full updated guidelines here.
CMS Releases Final 2025 Fee Schedule
CMS has finalized the 2025 Medicare Physician Fee Schedule, implementing a 2.83% cut to Medicare physician reimbursements, as previously outlined.
This cut continues a long trend of decreased reimbursements, originating with the Budget Control Act of 2011 under the Affordable Care Act. As a result, sequester cuts of 2% will remain in effect until 2032 unless Congress enacts a permanent fix to prevent these annual adjustments.
Impact on Interventional Pain Management (IPM) Services:
The final schedule reflects a 2.83% reduction in reimbursements for IPM services.
New Bipartisan Legislation Introduced to Counter Cuts:
Congressman Greg Murphy, M.D., has introduced a bipartisan bill to address this issue. This legislation aims to prevent the proposed reimbursement cut and introduce a payment increase (1.8%) equal to half of the Medicare Economic Index, aligning with recommendations from the Medicare Payment Advisory Commission.
The bill has garnered support from AMA, numerous organizations, including ASIPP. We encourage all members to act by contacting your congressman and senators to support this legislation.
ASC:
There are no major changes for IPM procedures in ASC settings, aside from adjustments in specific codes. Notably, there is a 2% to 3% increase for codes 62361, 62360, 61885, 64590, and 62362, while codes 63688, 64595, 63664, 64585, 63662, 64569, 62350, and 64553 will see a 5% to 7% decrease.
New ICD Codes Effective October 1, 2024
The new ICD-10 codes, effective October 1, 2024, must be implemented immediately to ensure proper reimbursement, including for UDS claims.
The following new codes have been developed:
M51.360: Other intervertebral disc degeneration, lumbar region with discogenic back pain only
Other intervertebral disc degeneration, lumbar region with axial back pain only.
M51.361: Other intervertebral disc degeneration, lumbar region with lower extremity pain only
Other intervertebral disc degeneration, lumbar region with leg pain only.
Other intervertebral disc degeneration, lumbar region with referred sclerotomal pain only.
M51.362: Other intervertebral disc degeneration, lumbar region with discogenic back pain and lower extremity pain
Other intervertebral disc degeneration, lumbar region with discogenic back pain and leg pain.
Other intervertebral disc degeneration, lumbar region with axial back pain and referred sclerotomal pain.
M51.369: Other intervertebral disc degeneration, lumbar region without mention of lumbar back pain or lower extremity pain
Other intervertebral disc degeneration, lumbar region without mention of lumbar back pain or leg pain.
Other intervertebral disc degeneration, lumbar region, NOS.
M51.370: Other intervertebral disc degeneration, lumbosacral region with discogenic back pain only
Other intervertebral disc degeneration, lumbosacral region with axial back pain only.
M51.371: Other intervertebral disc degeneration, lumbosacral region with lower extremity pain only
Other intervertebral disc degeneration, lumbosacral region with leg pain only.
Other intervertebral disc degeneration, lumbosacral region with referred sclerotomal pain only.
M51.372: Other intervertebral disc degeneration, lumbosacral region with discogenic back pain and lower extremity pain
Other intervertebral disc degeneration, lumbosacral region with discogenic backpain and leg pain
Other intervertebral disc degeneration, lumbosacral region with axial back pain and referred sclerotomal pain
M51.379: Other intervertebral disc degeneration, lumbosacral region without mention of lumbar back pain or lower extremity pain
Other intervertebral disc degeneration, lumbosacral region without mention of lumbar back pain or leg pain
Other intervertebral disc degeneration, lumbosacral region, NOS
M54.5: Low back pain
Excludes1: intervertebral disc degeneration, lumbar region with discogenic back pain only(M51.360)
intervertebral disc degeneration, lumbosacral region with discogenic back pain only(M51.370)
M54.3: Sciatica
Excludes1: intervertebral disc degeneration, lumbar region with lower extremity pain only(M51.361)
intervertebral disc degeneration, lumbosacral region with lower extremity pain only(M51.371)
M54.4 Lumbago with sciatica
Excludes1: intervertebral disc degeneration, lumbar region with discogenic back pain and lower extremity pain (M51.362)
intervertebral disc degeneration, lumbosacral region with discogenic back pain and lower extremity pain (M51.372)
However, these codes have not been updated with Medicaid, etc. Consequently, for facet joint pain the codes remain M47.816 and M47.817.
Similarly for radicular pain, lumbar radiculitis, M51.16 and M51.17 will remain.
See the following link to CMS: https://www.cms.gov/medicare-coverage-database/view/article.aspx?articleid=56818&ver=45&=
Updated Antithrombotic Guidelines Available!
The updated Antithrombotic Guidelines from ASIPP are now available! This 94-page publication includes 412 references, 23 tables, and 15 figures, and offers crucial insights based on extensive research.
CMS Proposes 2025 Physician Fee Schedule with 2.8% Reduction and Ambulatory Surgical Center Payment System with a 2.6% Increase:
Overall Bad News with Sequester Cuts Remaining in Place
1. Proposed 2025 Physician Fee Schedule
On July 10th, CMS released the proposed rule for the 2025 Medicare physician fee schedule (MPFS). Rule focuses on several key goals of administration, including addressing health disparities, expanding access to behavioral health care, improving transparency in health system, and promoting safe, effective, and patient centered care.
The highlights are as follows:
- The rule proposes to cut the conversion factor by 2.8% to $32.36 in CY 2025, as compared to $33.29 in CY 2024.
The cut reflects the expiration of the 2.93% statutory payment increase for 2024, a 0% conversion factor update, and a 0.5% budget neutrality adjustment.
In the past, Congress has avoided those cuts with an annual “doc fix” bill, and many lawmakers with whom ASIPP has been in contact, along with other organizations are seriously discussing a more permanent solution this year. It is a matter of resolve and transfer of money from one place to the other.
- The proposal rule also adds payment for G2211 (an add-on code per visit complexity) even in some instances when modifier 25 is used.
- Telehealth will be extended until December 2026, based on a bill in the Congress. https://www.congress.gov/118/bills/hr7623/BILLS-118hr7623ih.pdf
- Sequester Cuts
As we have been experiencing for several years since the Budget Control Act of 2011 for Affordable Care Act, sequester cuts will continue at 2% until 2032. This issue is also being considered by Congress for permanent fix without recurring issues each year.
- Effect on IPM Services
- Changes reflect 2.8% cut
2. Ambulatory Surgical Center Payment System
2025 Medicare hospital outpatient prospective payment system and ambulatory surgical center payment system proposed rule on July 10, 2024, emphasizes addressing health disparities, expanding access to behavioral healthcare, improving transparency in the health system, and promoting safe, effective, and patient-centered care.
Good news on the ASC part is that there is an increase in payment rates of 2.6%.
Again, this does not include 2% continuous sequester cut which we are working on permanently eliminating.
- Effect on IPM services:
As you see from the fee schedule, it appears that there will be following increases:
- 3.7% increase for epidurals, intercostal nerve blocks, sacroiliac joint injections, and spinal cord stimulation procedures.
- 2.5% increase for radiofrequency neurotomy procedures
- 1.5% increase for transforaminal and facet joint injections
Comments can be made on both policies and are due by September 9, 2024.
ASIPP members in good standing can access the complete fee schedules on the Members’ Only Website.

Extension of Telehealth Modernization Act of 2024
The Telehealth Modernization Act of 2024, a bipartisan, bicameral legislation, is progressing through Congress, which includes the following:
- Extension of certain telehealth flexibilities removing geographic requirements and expanding origination sites for telehealth services and extending them through the end of December 31, 2026 (was scheduled to expire 12/31/2024).
- This legislation also allows and extends audio only telehealth services, through December 31, 2026 (was scheduled to expire 12/31/2024).
This is great news for patients and providers to maintain access, convenience and to provide cost effective established evaluation and management services. The legislation has been sponsored by bipartisan members of Congress. If you recall, Dr. Larry Bucshon, a member of the Committee on Energy and Commerce and Congressman James Comer, Chairman of the Committee on Oversight and Accountability, discussed this extensively and worked on extending it further. While ASIPP has spearheaded to make this a reality, numerous organizations have worked tirelessly led by AMA.
The only deficiency is that it is not yet permanent. We will continue to work on this issue.
LATEST UPDATE
Medicare Revises LCD – Facet Joint Interventions for Pain Management (L38773) with Coverage for Therapeutic Facet Joint Nerve Blocks
Medicare publishes revised LCD for Facet Joint Interventions for Pain Management, providing coverage for therapeutic facet joint nerve blocks.
As you know, the LCD which went into effect on 5/2/2021, limited its coverage to intraarticular joint injections. When ASIPP became aware of this limited coverage, we began contacting Medicare to request a policy change to include therapeutic facet joint nerve blocks. After several correspondences, we were advised to file a reconsideration request. Our reconsideration request went through the appropriate channels and the LCD has been revised effective 7/7/2024, which includes medial branch blocks as a therapeutic procedure, along with the intraarticular injections.
Once again therapeutic facet joint injections or medial therapeutic facet joint nerve blocks are not covered unless there is justification in the documentation showing why radiofrequency neurotomy cannot be performed.
ASIPP was able to obtain this addition by presenting appropriate evidence with multiple systematic reviews as well as up-to-date literature. A presentation was also made by Dr. Laxmaiah Manchikanti and Dr. Amol Soin at CGS open meeting.
In addition to CGS, all MACs have either changed or are in the process of changing their policies. Please see the policy from CGS using the following link. https://www.cms.gov/medicare-coverage-database/view/lcd.aspx?LCDId=38773
Washington State Authority Health Care Authority Publishes Draft Findings Providing Coverage for Spinal Cord Stimulation
As some of you may know, Washington State Authority Health Care Authority has been considering coverage for spinal cord stimulation. Other states will be doing the same. ASIPP has been working on this for quite some time, along with multiple other organizations. Dr. Amol Soin and Dr. Chris Gharibo were intimately involved. Dr. Gharibo testified on our behalf in front of the Commission. Dr. Soin wrote the public comments. Overall, Washington State Authority Health Care Authority changed its policy, and the draft policy shows they are going to cover spinal cord stimulation for post lumbar laminectomy syndrome, non-surgical low back pain, and painful diabetic peripheral neuropathy, but not for complex regional pain syndrome.
Overall, this is very good, but we will have to overcome multiple limitations included in this, such as each patient undergoing the completion of a comprehensive cognitive behavioral therapy, chiropractic, or acupuncture, which seems to be impractical or extremely difficult to achieve. We are working on these issues, as well as with other organizations.
ASIPP congratulates all those involved in this great cause, which is largely moving in a positive manner. This is a big step forward considering that it was not covered at all.
Please find the Spinal Cord Stimulation DRAFT findings and decision: https://www.hca.wa.gov/assets/program/SCS-draft-findings-and-decision.pdf
Effective from April 1st, the Majority of MAC Will Follow Updated Guidelines for Trigger Point Injections
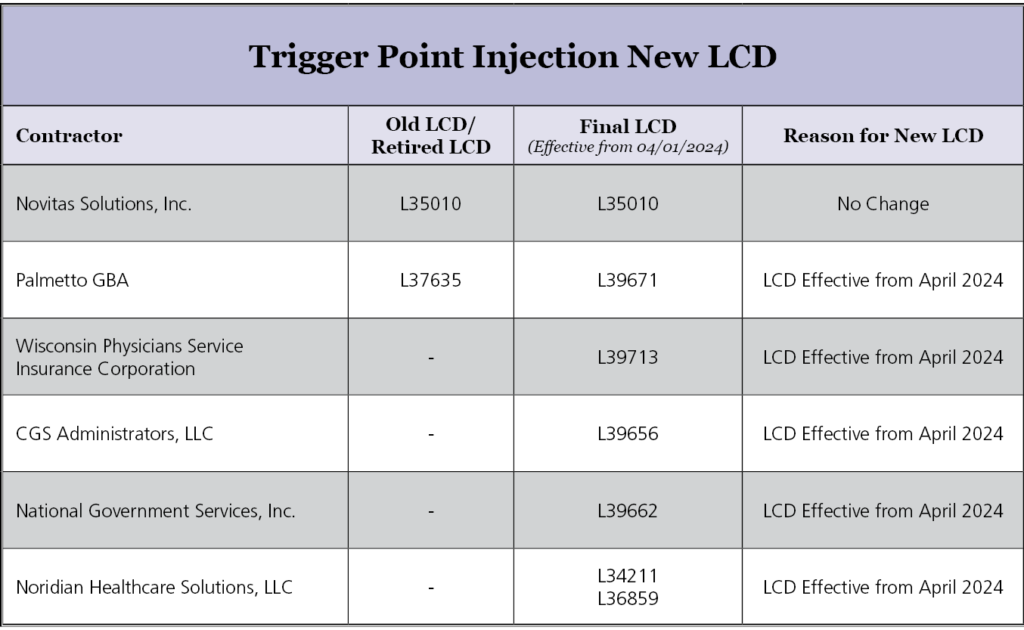
Effective from April 1st, the majority of MAC follows the above guidelines for Trigger Point injections.
Below are major points from the updated LCD:
• Frequency: No more than 3 TPI sessions will be reimbursed per rolling 12 months.
• Imaging guidance: The use of fluoroscopy or magnetic resonance imaging (MRI) guidance for the performance of TPI is not considered reasonable and necessary, The use of ultrasound guidance for the performance of TPI is considered investigational.
• Repeat TPI: Consistent pain relief from the most recent previous TPI lasting at least 6 weeks.
• With other Injections: It is not considered medically reasonable and necessary to perform multiple blocks (e.g., epidural steroid injection (ESI), sympathetic blocks, facet blocks, etc.) during the same session as TPI.
• Pain Scale: Documentation should be updated with the pre and post-pain scale.
Below are attachments for the updated LCDs:

Join the AMA or Renew Your Membership Today!
On behalf of the Board of Directors of the American Society of Interventional Pain Physicians (ASIPP), we ask that you help IPM to maintain a voice in the AMA. Please join the AMA or renew your membership today.
ASIPP previously had two positions in the House of Delegates (HOD), however we just learned that in our 2024 review, we did not have enough ASIPP members on the AMA roster to keep our second seat. Consequently, we now have only one position.
However, it is now time for our 5-year review of our membership AMA match. The member list we send to the AMA every five years is the list they use each year for five years to determine our status. This means that if we fall below the minimum requirement, we stand to lose our only remaining seat.
For ASIPP to retain our seat, the AMA requires that 20% of ASIPP’s physician members also be members of the AMA. ASIPP must submit our member list no later than Monday, April 15. Because of this, we ask that you check your AMA status and renew or join TODAY.
Joining the AMA will strengthen our specialty’s representation at the national level through the AMA HOD the AMA’s policymaking body, and strengthen our ability to meet the challenges in health care today with thoughtful, well-organized responses to issues such as Medicare payment cuts, medical liability reform, etc.
Membership also gives you access to a broad range of practice management resources and award-winning publications, such as the Journal of the American Medical Association, AMNews, AMA Morning Rounds and the Archives journals.
Please support the critical activities of ASIPP by joining the AMA today. To join or renew the AMA, click on the following link: Join or Renew Here.
CMS And Optum to Provide Accelerated Payment Loans and CMS Urges Medicaid Managed Care Plans and Medicare Advantage Plans to Offer Similar Loans
As reported last week, there was a cyberattack on UnitedHealth Group’s subsidiary Change Healthcare. Change Healthcare started experiencing major problems Feb. 21 cutting providers off from payer reimbursements.
Due to lobbying from various groups including ASIPP, temporary loans for all providers including physicians have been arranged. If you recall, this was limited to only hospitals in the beginning.
On Saturday March 9, 2024, CMS issued the attached statement announcing that in addition to considering application for accelerated payments for Medicare Part A providers, application for advanced payments for Part B suppliers will also be considered.
CMS issued a Fact Sheet with additional detail on eligibility requirements, certification terms, and payment amounts.
All MACs will provide public information on how to submit a request for a Medicare accelerated or advanced payment on their website starting March 9, 2024.
CMS is also urging Medicaid Managed Care Plans and Medicare Advantage Plans to offer similar emergency payment loans to cope with Change Healthcare cyberattack.
In addition to the CMS program of accelerated payments, United Health Groups loan program administered through Optum Financial Services offers financial assistance to providers whose payer payment are processed through Changes EDI. The loan amount is based on average prior claims volume and how much the provider’s payment distributions have been affected. No interest or fees will be charged, but the funds must be repaid.
Overall, while this may help physicians who were excluded in the beginning, it may not be sufficient. Many practices are seeing that a mere fraction of the daily deposits are being given in the form of loans.
If you have any questions, contact your MAC, as well as Optum, your representative for United Health Group or Optum for assistance.
MORE ON Chane Healthcare Cyberattack can be found on the following websites:
MedScape – AMA – HHS – TechTarget – CMS
U.S. Congress Finally Reduced the Cut by Half 1.68% from 3.37% Effective March 9, 2024
In a federal budget deal struck to avoid a government shutdown, the House of Representatives has voted to reduce about half (1.68%) of the 2024 3.37% across-the-board physician pay cut that took effect in January. The Senate is expected to vote soon, and the President is expected to sign which will be effective March 9.
This essentially means Congress has again failed to stop in its entirety a pay cut that threatens Medicare patients’ access to high-quality physician care.
The cut continues to persist over 2% of sequester cuts totaling to 3.68%, on top of 4% from last year’s physician pay reduction. Unfortunately, as in contrast to prior years, this payment rate is not retroactive.
This was achieved due to enormous effort by all organizations, including ASIPP, with widespread support to block the 3.37% Medicare cuts for physician services on a permanent basis.
Our conversations with members of Congress show that they are looking at ways to create a permanent fix for these issues. We need to continue to place pressure on Congress for a permanent fix. The graph below shows 2024 Medicare payment updates prior to the 50% reduction of the cut as projected by AMA. The only change would be 1.68%. instead of 3.4%.
Officials Rush to Help Hospitals, Doctors Affected by Change Healthcare Hack
Federal officials and health-industry executives Tuesday said they were racing to help hospitals and health-care providers that are at risk of running out of cash after a cyberattack knocked out the nation’s largest processor of medical claims and put pressure on patient care.
The Department of Health and Human Services unveiled a strategy that encouraged private health plans to advance funding to the hardest-hit organizations and relax requirements that often slow the billing process, among other steps. The Centers for Medicare and Medicaid Services (CMS) said it would consider individual requests for accelerated payments, akin to those made during the coronavirus pandemic, recognizing that “hospitals may face significant cash flow problems from the unusual circumstances impacting hospitals’ operations.”
Aledade, the nation’s largest network of independent primary care practices, also announced that it would advance up to $100 million to its physician practices across the country.
Read More: https://ow.ly/2bpk50QOJG3
The Saga of Amniotic Tissue Intraarticular Injections
is Coming to an End
As you recall, ASIPP sent a news alert on October 29, 2020 focusing on Q codes and potentially fraudulent billing with intraarticular injections. ASIPP also sent a letter to Medicare MAC directors on November 3, 2020.
After the time of this alter, there have been incidences of fraud and abuse. Recently, a physician assistant went to trial in Fort Worth, TX and was convicted at this trial. Dr. Manchikanti provided the testimony for the Department of Justice highlighting the news alert from ASIPP.
The trial lasted 5 days. Subsequently, in less than 1 hour of deliberation, a jury convicted Ray Anthony Shoulders on all counts.
It is important to ASIPP and crucial to protect our physicians from fraud and abuse investigations, and at the same time, protect the Medicare program.
Important News Alert on Disastrous Reductions Due to a Computer Glitch for ASC Payments
On January 2nd, 2024, an ASIPP member from Texas brought to our attention a concerning issue, a 46.1% reduction in all ASC payments. This unexpected news prompted immediate action on our part. Acting swiftly, ASIPP and SIPMS reached out to CMS through the office of Cathy McMorris Rodgers, Chairman of the Energy and Commerce Committee, and CGS MAC Directors by ASIPP and SIPMS, seeking resolution.
CGS, led by Earl Berman, MD, promptly addressed the matter, successfully rectifying and adjusting the rates within 24 hours. All other MACs are still correcting.
Additionally, we want to inform you that a sample table has been generated for Kentucky’s McCracken County.
While Noridian, Novitas, NGS, Palmetto GBA, and WPS still reflect rates at 54% of the National Price, we intend to wait for 24 hours then contact them to expedite the resolution of this issue.
ASIPP UPDATES
ASIPP is pleased to announce the publication of the Comprehensive Evidence-Based Guidelines for Epidural Interventions in the Management of Chronic Spinal Pain. In preparation of the guidelines, an extensive literature review was performed. The 210-page guidelines contains 33 figures, 48 tables, 1,345 references and has 60 authors.
In addition to the review of multiple manuscripts in reference to utilization, expenditures, anatomical and pathophysiological considerations, pharmacological and harmful effects of drugs and procedures, for evidence synthesis, we have included 47 systematic reviews and 43 RCTs covering all epidural.
[ READ MORE ]
ANNOUNCEMENTS

[ LOGIN | JOIN ASIPP ]
Members Only Resource
[ CLICK TO VIEW ]

Doctor Finder allows you to search for an ASIPP® Member Interventional Pain Physician anywhere in America by name or by location. It’s quick and easy.
Since this malpractice insurance program officially launched in November 2018, ASIPP has signed up hundreds of providers with an average savings of 30%. This is professional liability insurance tailored to our specialty and will stand up for us and defend our practices.
Curi is a full-service advisory firm that serves physicians and their practices. Their valued advice is grounded in your priorities and elevated in your outcomes. They are driven by a deep understanding of your specific circumstances in medicine, business, and life. To read a few important points to keep in mind about the program, including discounts, administrative defense, cyber coverage, aggressive claims handling, and complimentary risk management CME activities, click here.
PainExam is proud to announce that it now offers preparation for the ABIPP Pain Management Board Exam! In addition, PainExam has now collaborated with ASIPP to offer Virtual Learning programs.
[ READ MORE ]

PainCast, the pain management network, has collected years worth of information on the history and processes of the pain management specialization and transformed it into a virtual library of videos, journals, articles, podcasts, and more – all at your fingertips.
Essentials of Regenerative Medicine in Interventional Pain Management is a book to bring concise, collective, and comprehensive information to interventional pain physicians practicing regenerative medicine with its applications in managing chronic pain.
[ READ MORE ]
ASIPP has formed a partnership with Henry Schein and PedsPal, a national GPO that has a successful history of negotiating better prices on medical supplies and creating value added services for the independent physician.
[ READ MORE ]

ASIPP is now offering our members the benefit of a unique revenue cycle management/billing service. We have received a tremendous amount of interest in the ASIPP billing and coding program.
[ READ MORE ]
